This was my first USCHA (US Conference on HIV/AIDS), and I wasn’t ready for it. I’ve been to HINAC (HIV Is Not a Crime) and AIDS Watch each twice, but this was different. There’s a magic at USCHA that gets under your skin.
I travelled to USCHA as part of NMAC’s 50+ Cohort, joining others like me from around the country who are aging and living with HIV. I’m grateful for the experience and the connections I made.
I’m 57. I’ve been living with HIV for 13 years. That’s my place in the timeline. Not better, not worse – just mine. But when I saw the decades of HIV/AIDS laid out at the Friday plenary, the science, the struggle, the survival – it cracked something open in me. For the first time, I felt the weight of what it means to be a long-term survivor. And I also knew that wasn’t me.
I came along after protease inhibitors, after HAART reshaped the fight. When I was diagnosed in 2012, my doctor told me, “The guidance is changing. We used to tell people to wait. Now we recommend you start treatment right away.” He still gave me the option – that’s how new it was. I didn’t understand then how historic that moment was. I do now.
In the 80s, I was a teenager. In the 90s, I was climbing the corporate ladder, coming out of the closet, largely disconnected from my community. By the time I came out, the epidemic wasn’t invisible anymore, but it was still tearing through our communities. The mid-90s would become the deadliest years. And while that grief was swallowing a generation, I was safe in my bubble, largely untouched, largely unaware. That’s the part that haunts me. The loss I didn’t live. The fire I didn’t feel.
So no – I don’t carry the same survivor’s guilt as those who were told they would die and somehow lived. My guilt is different. It’s the guilt of surviving in a post-HAART world, of being shielded by privilege, of waking up to a history I wasn’t part of, but which shaped everything around me.
At USCHA, no one made me feel like an outsider. But I did. I think people at USCHA saw me at 57 and assume I’m a long-term survivor. I’m not. I’m someone aging with HIV, without that same story. That difference is mine to wrestle with.
And yet, USCHA gave me clarity. It gave me a way to honor what came before me and what is still unfolding now. Because just as I look back in gratitude, I also look forward, knowing that those who come of age in the U=U and PrEP era will have their own place in history, too.
To say USCHA was “life-changing” sounds cliché. But this was something deeper. A reckoning. A reminder that every place in the timeline matters, including mine. And for that – for the people who came before me, for the community that still carries me forward – I am deeply grateful.
Keep telling the story,
Professor Peacock
Note: These are my thoughts and my story. I used AI to make helpful edits to my ramblings and online journaling.
When I was first diagnosed with HIV in 2012, the idea of seeing anyone other than an infectious disease specialist would have felt reckless, even dangerous. This was before PrEP, before U=U. Specialists were the gatekeepers – the people who knew the ever-changing science, the ones who gave me the sense of being in the safest possible hands. For a long time, they were the difference between life and death.
So when I learned today at my routine HIV lab follow-up that the Damien Center is shifting away from relying on infectious disease doctors, and instead training primary care physicians to handle HIV, my first reaction wasn’t celebration. It was shock. Fear. Even a little sadness. A part of me wanted to feel special, to believe that my care required the highest tier of expertise, that my condition set me apart in a way that demanded more than “just” primary care.
But sitting with that discomfort, I realized something important: this change is a milestone.
It’s not about being less cared for. It’s about HIV care becoming ordinary in the best possible sense. What was once an emergency requiring specialists is now a chronic condition that can be managed alongside everything else. Just like diabetes, high blood pressure, or asthma. And just as most people with diabetes don’t see an endocrinologist every month, most people living with HIV don’t need an infectious disease doctor at their side for every check-up. We need skilled, compassionate primary care providers who are equipped with the right training. That’s exactly what this new model is delivering.
The truth is, the biggest factors in HIV health today aren’t whether you have access to a specialist; they’re whether you can access care at all, whether your doctor treats you with dignity, whether you have support for housing, food, mental health, and transportation. Medicine has advanced so much that the day-to-day fight isn’t with the virus itself – it’s with the systems that surround care. And if we’re honest, it’s with stigma itself. Stigma kills.
When I was first diagnosed, I was in the hospital. A case of misdiagnosed stage-2 syphilis landing me in the ER. Thankfully, my visit to the ER is the reason I was diagnosed so soon after being exposed to the HIV virus. My infectious disease doctor told me they caught my HIV very early – he only saw a handful of cases each year like mine. I was lucky to be in his hands.
Around the time I was diagnosed in 2012, newer medications were available, and the medical advice began to shift towards starting treatment right away. Why? Because the side effects of the latest antiretroviral treatments (ARTs) were much milder, making it smarter to begin medication quickly to lower the viral load. This was all before the idea of U=U was introduced.
So, I’m very thankful for my infectious disease specialist, because he caught me “on the forefront of change.” Looking back, that was huge step forward.
Now, 13 years later, the fact that I don’t “need” one anymore isn’t a downgrade — it’s proof of progress. It means that medications work so reliably, and outcomes are so good, that HIV can finally be seen for what it is: not a death sentence, but a manageable chronic condition.
Of course, specialists still exist for rare or complicated cases – and that’s important. But the default has shifted. HIV no longer requires a small elite circle of experts. Instead, it belongs in the hands of everyday doctors, woven into the fabric of routine healthcare.
That’s not loss. That’s victory.
So yes, there was some grief in letting go of the idea that I needed a specialist. But in the end, this shift means something profound:
I am not defined by HIV. My care is not extraordinary because of this virus.
This disease is not terminal. It’s ordinary.
And that’s extraordinary.
Keep tellin’ the story,
Professor Peacock
Note: These are my thoughts and my story. I used AI to make helpful edits to my ramblings and online journaling, including some organization to be more blog-friendly.
I recently met a young college student who is living with HIV. It became apparent that he was interested in opportunities to get connected to the local HIV community, and didn’t know where to start or where to ask.
In some of the HIV community work I do, we’ve talked about two needs.
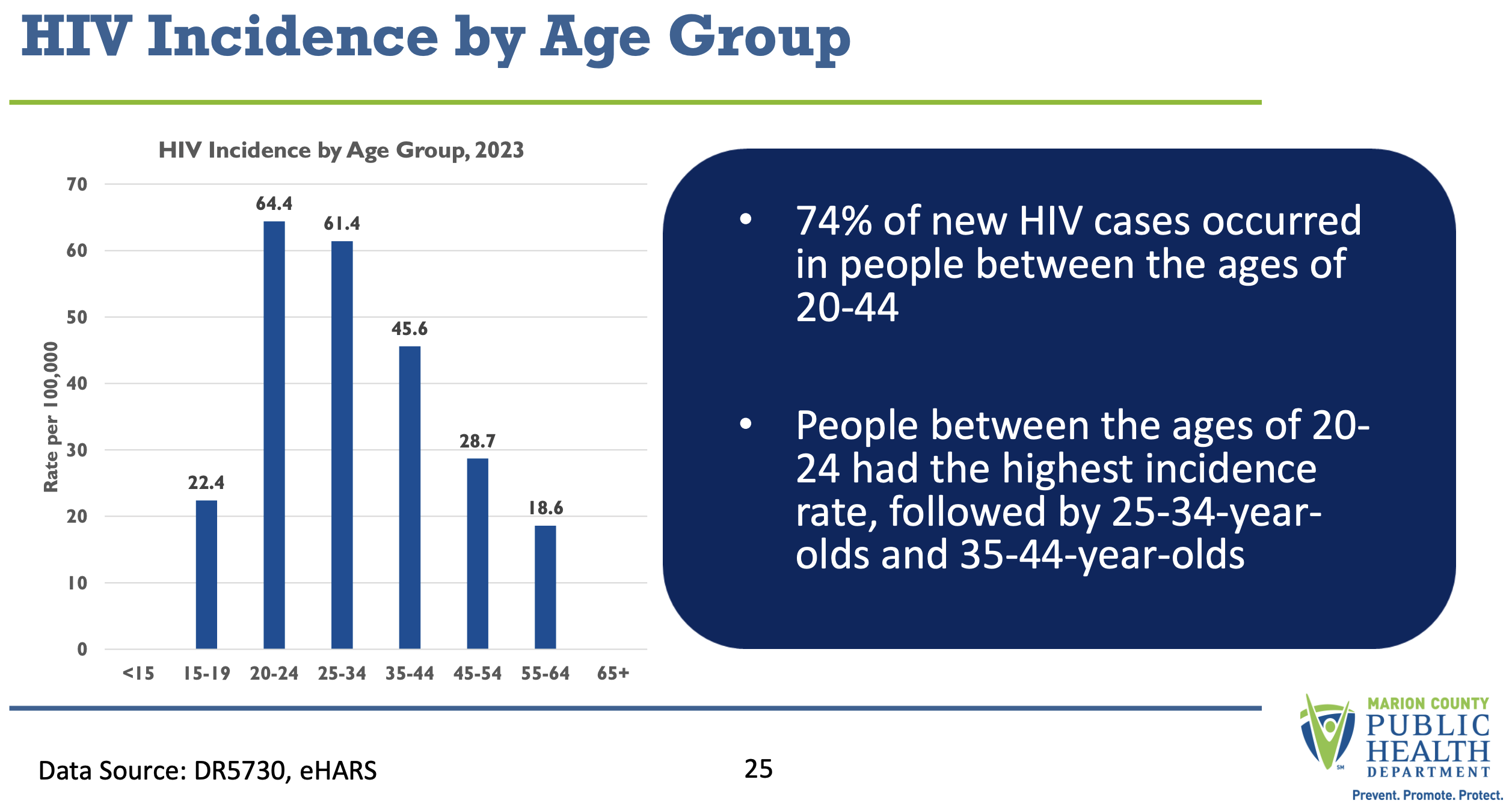
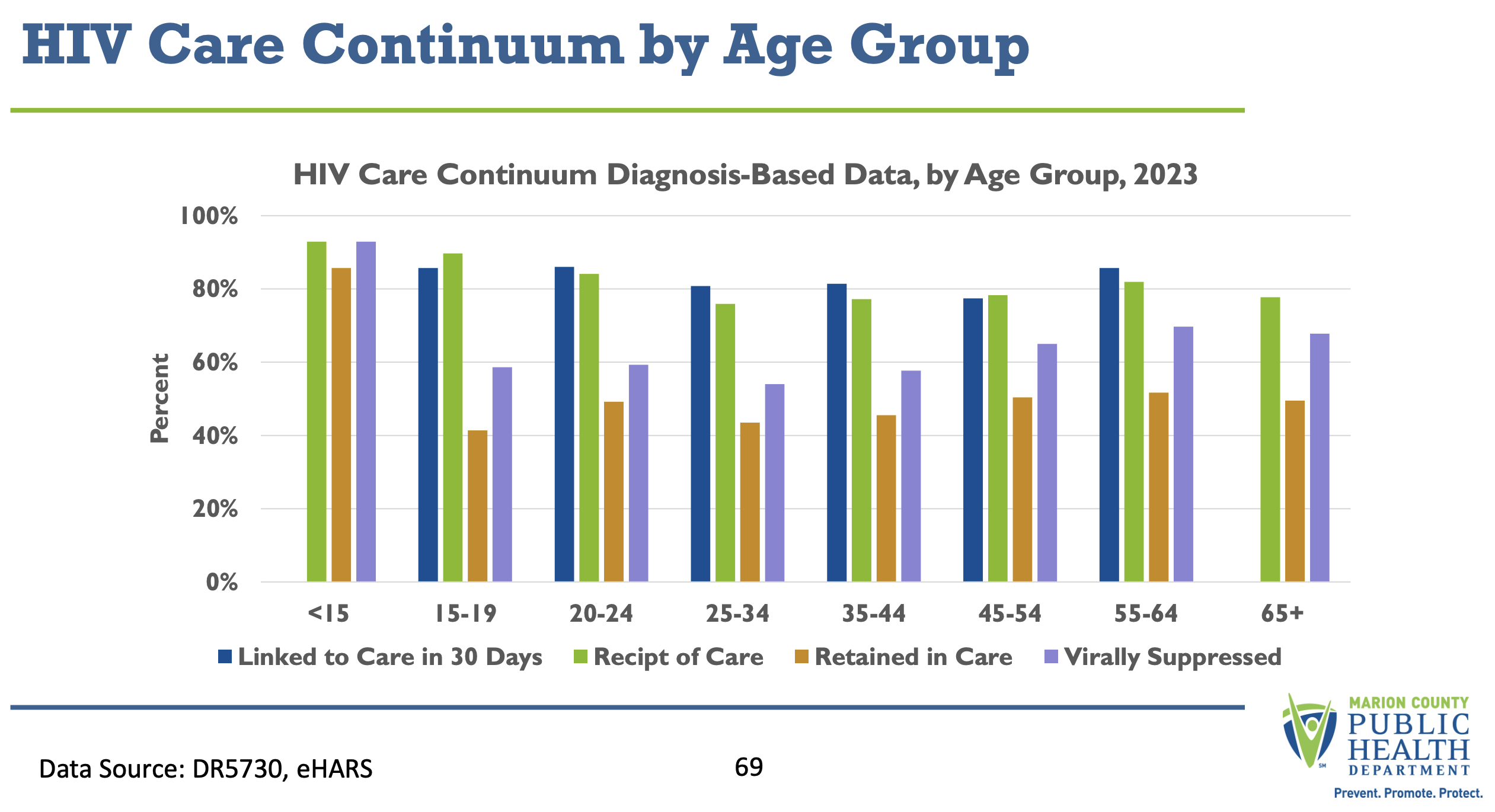
First, how do we better engage young people, because the highest rate of new cases in Marion County is ages 20-24 (see first graph below). We struggle to engage this age bracket! What are their unique needs? What are their unique challenges and opportunities? We also see the lowest retention in care and viral suppression rates for ages 25-34. We’ve got to do better prevention (including PrEP & testing) and engagement in care — doing so in culturally and ethnically accessible ways. WE MUST DO BETTER. (Source: 2023 Marion County HIV Epidemiology Profile
The second thing we struggle with is representation of this demographic in our community engagement and oversight – and really, all of the people under our care. In these cases, representation matters. So for example, we need people living with HIV to be on state, regional and local level councils and task forces. And within those councils, some are actually mandated by legislation that we have demographic representation.
These efforts represent partnerships between state and local level health departments, HIV care agencies & hospital systems, community organizations in the HIV arena and outside the HIV arena, including blood banks, plasma centers, faith-based organizations, places of worship etc. In these spaces, representation matters.
In our EHE Task force, we’ve been talking about creating a general presentation that could be taken to agencies and shared with people living with HIV. Rather than each committee or council coming to make the pitch, present them all at once! Educate and empower people on ways to get involved and have their voice heard. Hence, the idea for this blog post was born! It may lay the groundwork for a powerpoint or reel that can be shared. Thanks Obama!
Renewed HOPE – HIV Opportunities for Passionate Engagement
Given these two needs, I wanted to share as much information with this young man as possible – and then let him pick what makes most sense for him. In doing, I gave him “new hope and even more to be excited about in the future.” For me, meeting him and pulling this together for him gave me a “hope boost” as well. So, I came up with the acronym HOPE – ways to get involved in the HIV community that provide Helpful Opportunities or HIV Opportunities for Passionate Engagement.
Sadly AI misspelled my tagline – (subtle way of giving AI credit! The text of this post was written by me, no help from AI! But, I’m not a graphic designer!) AI helped me write the “meta description” for Google. Just to be clear 😉
I became very excited and wanted to share with him all the ways that he could get involved without overwhelming him.
This is written with a heavier emphasis (details) on opportunities in the Marion County area, or greater Indianapolis and surrounding counties. But, I’ll do my best to represent state and regional level groups – though I may need more help / time with the details on how to join. This is a start!
SUPPORT GROUPS
Phoenix Support Group@ BU Wellness – The Phoenix Group is a support group for those living with HIV. This group celebrates the resiliency and strength of people living with HIV while providing a safe space for authentic discussions. Phoenix Groups meets the second and fourth Thursday of every month at 5:00PM at BU Wellness 1712 N. Meridian. Contact Kem Moore at kmoore@buwellness.org for more information or just show up!
Sisters United@ BU Wellness – A safe space for Black/African American women living with HIV. Sisters United meets the second and fourth Wednesday of every month at 5 PM at BU Wellness 1712 N. Meridian. Contact Aminata Tounkara at atounkara@buwellness.org for more information or just show up!
Long Term Survivors @ Damien Center – The Positive Living Social Group is a space for those living and thriving with HIV to find peer support, share their journey, and connect with their community. Meets every week on Tuesday from 11a-12:30pm in the Damien Board Room. Contact: Robin Thompson (rthompson@damien.org) or just show up!
ADVOCACY / COMMUNITY WORK
Giving back feels good. But it’s also a way of making a difference, by being involved in various councils, task forces and coalitions. And as a I mentioned before, representation matters. Meaningful involvement of people with HIV/AIDS (MIPA) is about ensuring that the communities most affected by HIV are involved in decision-making, at every level of the response. Learn more about MIPA here.
Note: Some opportunities are volunteer; some offer a small stipend for PLWH’s time.
HIV Modernization Movement – Indiana – Statewide grassroots effort of PLWH and allies to modernize HIV criminal laws in Indiana. We introduce legislation each year to modernize HIV criminal laws that contribute to HIV stigma and are contrary to good public health. Join online to get monthly newsletters. Easy engagement – sign up at https://hivmodernizationmovement.org/join-us/
State-Level HIV/STI/Hep C Advisory Council – Indiana HIV/STI/Viral Hepatitis Advisory Council work in partnership with Indiana Department of Health to lead statewide efforts in identifying, implementing, and evaluating strategies and prioritizing funding to close gaps, eliminate barriers, and increase access to information, resources, supports, and services designed to end the HIV epidemic and eliminate Hepatitis C and STIs addresses any gaps, barriers or trends related to service provision in alignment with the Integrated Plan, Care Continuum and the ZIP IN Plan and provides advisement and guidance to IDOH. Council meets every other month to manage council business. There are various committees and ways to get more involved. More info at https://www.zipindiana.org/statewide-advisory-council
Regional ZIP (Zero is Possible) Coalitions – Zero is Possible – Indiana (ZIP-IN) is a statewide initiative bringing together the essential people, tools, and resources to end the HIV epidemic and eliminate Hepatitis C (HCV) in Indiana. Coalition meets 1.5 hours, once per quarter. Sign up at https://www.zipindiana.org/get-involved
Marion County Ending the HIV Epidemic (HIV) Task Force – The Ending the HIV Epidemic Task Force will maximize the authentic engagement of the community, especially priority populations, to end the HIV epidemic in Marion County. The Task Force meets 2 hours every other month. There are various committees and ways to get more involved. More information at https://marionplan.org/
County or Regional CAG (Community Action Groups) – I’m tired, and less familiar with these outside of Marion County. But there is funding and structures for local health departments to connect with local agencies and people living with HIV.
Client Advisory Board at your HIV clinic or agency – talk to your care coordinator, but each HIV service agency is required to have some form of client involvement or feedback. Many agencies use a client advisory board.
Volunteer at your agency – including being on their Board of Directors
Organ Donorship – sign up to be an organ donor! People living with HIV can have organs donated to other people living with HIV under the HOPE Act of 2013 (Congress). The HOPE Act has given more than 350 people living with HIV the opportunity to receive a transplant from an HIV-positive donor, with the first patients receiving transplants in 2016. Sign up here or at your local driver’s license branch!
I would recommend picking 1 to start with – there are a LOT of ways to engage, depending on what you’re looking for. Each board or meeting has its pros/cons, sphere of influence. I’m happy to share more if you want to know more.
A good place to start? Sign up for HMM-Indiana, and see what else your time allows!
CAREERS IN HIV CARE
There are two exciting opportunities I want to share: The Indiana Statewide AmeriCorp Program and the Marion County HIV Peer Navigator Program.
The Public Health AmeriCorps Program
The Health Foundation of Greater Indianapolis, Inc. currently supports a statewide Public Health AmeriCorps (a Healthy Futures grant supported by CDC) supporting up to 34 Members in partnership with 18 Service Sites, located in every region of Indiana. Our program is focused on development in under-resourced areas that will benefit from further enhancement of public health infrastructure, as it relates to HIV, Hepatitis C (HCV), and Harm Reduction. Lived experience is encouraged but not required. This program last for 11 months (September-July), and provides a living stipend. For more information including applications go to https://thfgi.org/americorps/
Information for 2024/25 Year (subject to change in the future)
🗓️ Full-time service from September 1, 2024, to July 31, 2025 💰 Living allowance up to $20,000 🎓 Education Award of $7,395.00 👩⚕️ Comprehensive health, dental, and vision insurance 👶 Childcare assistance and loan forbearance options 📚 Extensive training, mentorship, and professional development opportunities 🤝 Make a difference while gaining valuable experience in public health and community service!
Marion County HIV Peer Navigator Program
A new grant-funded program starting in 2024, that will provide 3+ HIV Peer Navigators in Marion County. This is the first HIV Peer Navigation program in the State, as far as I’m aware. This has been successfully implemented in Florida, Illinois and many other locations. This position plays a pivotal role in helping engage or re-engage persons living with HIV, PLWH, into treatment and care programs. This position will engage, coach, and mentor clients in developing skills needed to ensure treatment retention, medication adherence, and viral suppression. The first 3 positions were hired in August 2024, so as it expands or there is turnover, there may be new opportunities. This is a paid opportunity with benefits – a great entry level position for someone wanting to work in the field. Although the Health Department can’t state this as a requirement because of HR policies, the intent is to fill these positions with individuals living with HIV. This approach is modeled after success in the addiction/recovery arena, and has been successful in other states and cities.
KEY ANNUAL EVENTS & FUNDRAISERS
Again, these are largely Indy-area hosted, although some are statewide (e.g. UNITY) and several try to draw statewide participation for award presentations.
Spotlight– fundraiser for Indiana AIDS Fund (April)
Long-Term Survivors Day Event – hosted by BU Wellness Network (on or around June 5)
Zero HIV Stigma Day Event – hosted by HIV Modernization Movement – Indiana. Learn why people attended the event through an online art intervention. Click here to learn more. (on or around July 21)
UNITY – statewide HIV/STI/HepC Conference, hosted by IDOH (every other year in September)
Indiana AIDS Walk– The annual Indiana AIDS Walk, held in the fall of each year, supports the Gregory R. Powers Direct Emergency Financial Assistance (DEFA) program. The Indiana AIDS Walk raises more than $175,000 to help Hoosiers living with HIV/AIDS pay for medication, transportation to and from doctor’s appointments, dental bills, rent and utility bills, and even food and clothing in emergencies. (September)
Annual World AIDS Day Celebration hosted by Indianapolis Urban League’s (IUL) (on or around December 1)
Keep HOPE alive, give back & pay it forward! Volunteering matters.